

KEY TAKEAWAYS
- Closed comedones respond to BHA (salicylic acid). Milia do not. Extracting milia causes scarring
- Keratosis pilaris on the face needs lactic acid, not salicylic acid. The keratin buildup needs a different fix
- Textural dehydration looks bumpy but improves with humectants, not exfoliation. Scrubbing makes it worse
- Comedone-causing ingredients hide in moisturisers and SPF, not just foundations
- Heavy occlusive creams around the eye area are a leading trigger for milia
- If bumps are perfectly round, hard, and won’t squeeze out, they are milia. Stop trying to extract them
- KP affects around 40% of adults worldwide. It has no cure but responds well to consistent treatment
What causes rough bumpy skin that isn’t acne?
The four most common causes of rough bumpy skin texture that are not standard pimples are: closed comedones (clogged pores where sebum is trapped under the skin surface), milia (small keratin cysts just below the skin), keratosis pilaris on the face (excess keratin blocking hair follicles), and textural dehydration (lack of water in the skin’s outer layers). Each type looks different, responds to different treatments, and gets worse with the wrong approach.
You’ve tried spot treatments & bought every acne product on the shelf. Your skin is still rough, bumpy, and nothing is clearing it. The reason might be, what you’re treating isn’t acne at all.
Rough bumpy skin texture, small white bumps that won’t budge, flesh-coloured bumps sitting in clusters in your T-zone, are four completely different skin conditions, and each one needs a completely different fix. Using acne treatments on the wrong type doesn’t just fail. It often makes things worse.
I spent months treating what I thought were pimples with benzoyl peroxide and salicylic acid before realising they were something else. The skin texture not pimples conversation is one nobody has enough.
This guide covers the four main types of small bumps that aren’t standard acne, how to tell them apart visually, what causes each, and what actually works for each type.
Why Identifying the Type of Bump Matters Before Treating It
Treating the wrong type makes things worse
Most people see a bump and reach for whatever worked on their last breakout. That makes sense until you realise that milia cannot be dissolved or exfoliated away. They’re keratin cysts sitting below the skin surface. Applying acids to them does almost nothing, and aggressive squeezing pushes the keratin deeper and risks permanent scarring.
Patient.info says milia are harmless and typically resolve on their own, but the wrong treatment including attempting home extraction can cause skin damage that takes far longer to heal than the milia itself would have.
Keratosis pilaris on the face is just as misunderstood. BHA (salicylic acid) is excellent for clogged pores but for KP, lactic acid works better because it softens the keratin buildup that’s actually causing the problem. Using the wrong one for months means no results.
The visual checklist: size, colour, feel, and location
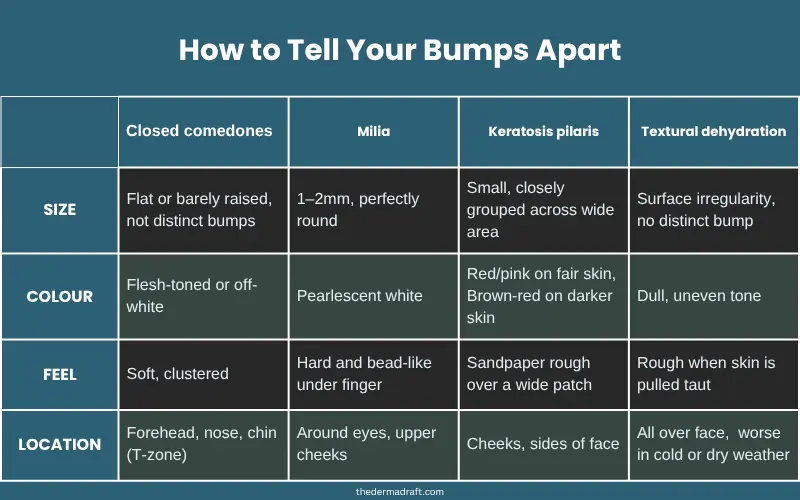
Before doing anything else, look closely at the bumps in natural light. Milia are typically 1 to 2mm, perfectly round, and very hard. Closed comedones are flatter, grouped in clusters, and barely raised. KP bumps feel rough and sandpaper-like across a wider area rather than sitting as individual spots.
Colour gives clear clues. Milia are pearlescent white. Closed comedones are flesh-coloured or slightly off-white. KP bumps tend to look red or pink on fair skin and brownish or red-brown on medium to darker skin tones. That detail matters and most guides skip it entirely.
Location also narrows things down. KP appears on the cheeks and sides of the face. Closed comedones cluster around the forehead, nose, and chin. Milia show up most around the eye area and upper cheeks.
When to stop self-treating and see a dermatologist
If you’ve been treating bumps consistently for 8 to 12 weeks with no change, or if they’re painful, spreading rapidly, or leaving marks, it’s time to see a dermatologist. Some conditions, like deep milia or folliculitis, need professional extraction or prescription treatment that no over-the-counter product can replicate.
Type 1: Closed Comedones (Congested Pores)

What they are and what they look like
Closed comedones are clogged pores where sebum gets trapped underneath the skin surface. Unlike blackheads there’s no opening. The skin grows over the plug. They appear as small, flesh-coloured or slightly white bumps that are flat or barely raised, usually grouped in the T-zone: forehead, nose, and chin.
DermNet NZ says closed comedones are among the most common forms of non-inflammatory acne and are primarily caused by follicular plugging, a combination of excess sebum and incomplete shedding of dead skin cells.
What causes closed comedones
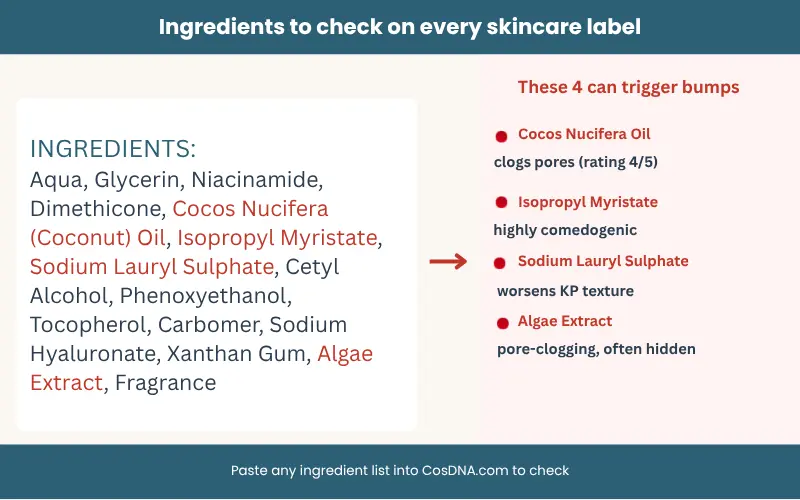
The two biggest causes are comedogenic ingredients in your skincare and insufficient exfoliation. Coconut oil, isopropyl myristate, certain silicones, and heavy butters are among the most common pore-clogging ingredients and they hide in moisturisers and SPF far more often than you’d expect. Many of these products are even labelled non-comedogenic, a claim that has no legal definition and means whatever a brand decides.
Your SPF is the most likely culprit. It sits on your skin all day while your cleanser rinses off in seconds.
How to treat closed comedones
Study indexed on PubMed confirmed that salicylic acid penetrates into the pore lining due to its oil-soluble and keratolytic properties, dissolves the plug, and helps prevent new ones forming. Start slowly at two to three times a week, not daily.
You can use CosDNA.com to check ingredients in your products. Paste the ingredient list in and it flags pore-clogging ingredients by severity. It takes two minutes. For a deeper look at hidden product triggers, the guide on why you’re still breaking out with a consistent skincare routine covers exactly what to audit.
Type 2: Milia (Keratin Cysts)
What milia actually are
Patient.info classifies them as cysts, not a form of acne, infection, or allergic reaction.
Visually, they’re distinct once you know what to look for: perfectly round, hard, pearlescent white, about 1 to 2mm wide, appearing most often around the eyes, upper cheeks, and nose.
They don’t have a head like an inflamed whitehead. They feel smooth and firm, almost bead-like when you press gently.
Why you should not try to extract milia at home
They will not come out with squeezing because there is no natural opening in the skin above them. Pressing harder pushes the keratin deeper causes bruising and inflammation and can leave scarring.
DermNet NZ says milia are best left alone or treated by a trained professional. Gentle chemical exfoliation can help the skin shed more regularly and prevent new milia from forming over time, but it won’t remove existing ones.
What actually helps
Most milia resolve on their own within a few weeks to a few months if you stop irritating the area. Remove heavy occlusive creams from around the eye area, which are a primary trigger. Introduce gentle chemical exfoliation a few nights a week using lactic acid or glycolic acid. For persistent milia, professional extraction using a sterile lancet is the safest and most effective option.
Type 3: Keratosis Pilaris on the Face

The keratin connection
Keratosis pilaris is a genetic condition where excess keratin builds up around hair follicles, blocking them and creating rough, bumpy texture. It’s not contagious, not caused by poor hygiene, and has no permanent cure. What it can do is respond well to consistent treatment.
Keratosis pilaris affects approximately 40% of adults and up to 80% of adolescents worldwide( StatPearls (National Institutes of Health) ). Many spend years treating it as acne without ever getting results.
What KP on the face looks like
On fair skin, KP bumps typically appear red or pink. On medium to darker skin tones, they look brownish or red-brown, often with slight darkening around them.
This distinction matters because most images online show KP on pale skin, which means a large proportion of people with medium or darker complexions don’t recognise it.
The texture is the main tell: rough, sandpaper-like, usually across the cheeks or sides of the face. The bumps are small and closely grouped, not spread out individually the way hormonal spots are.
Keratosis pilaris face treatment that actually works
AAD supports consistent AHA use as one of the most effective approaches for managing KP texture over time.
Avoid physical scrubs and sodium lauryl sulphate (SLS) because SLS strips the skin barrier and worsens the texture. Gentle, consistent exfoliation over several weeks is what shifts KP, not aggressive scrubbing. If you’re not sure whether your cleanser contains SLS or how to check, why every cleanser causes skin redness breaks down exactly how to read a label for surfactant type
Type 4: Textural Dehydration
How dehydration creates bumpy skin texture
Textural dehydration is probably the most misunderstood condition on this list. It’s not a structural issue like keratosis Pilaris. It happens when the outer layers of your skin don’t have enough water. The surface becomes irregular, rough-feeling, and uneven in a way that looks and feels like bumps.
Skin surface irregularity increases significantly with transepidermal water loss. As the skin loses moisture, its texture visibly worsens. It’s a direct link between hydration and texture that’s often missed when people focus on treating congestion.
The scrubbing mistake most people make
When skin feels rough and uneven, the instinct is to exfoliate. This is exactly the wrong move for dehydration-driven texture. Exfoliating already-dehydrated skin strips away what little barrier function remains and creates a cycle where the skin gets rougher, not smoother.
There’s a simple visual test: gently pull your skin taut. If the texture becomes more visible when stretched, that’s dehydration. Dehydration-related texture also worsens in cold or dry weather and improves in humid conditions or after a warm shower.
Rough skin plus a dry climate almost always means dehydration. Reach for hyaluronic acid before you reach for an exfoliant.
How to fix dehydration-related texture
Humectant-rich products are the fix. Hyaluronic acid and glycerin draw water into the skin’s surface layers. Apply them to slightly damp skin then seal with an occlusive moisturiser (something with shea butter, squalane, or ceramides) to lock that moisture in. Internal hydration matters too.
Morning skincare vs night skincare guide explains the right order for both AM and PM routines.
Skincare Products That Trigger Each Type
Knowing what causes each type also means knowing which products to avoid. Here’s a quick reference that covers the most common triggers, including some that hide in products you’d never suspect.
| Bump Type | Trigger Ingredients | Commonly Found In | What to Do |
| Closed Comedones | Coconut oil, Isopropyl Myristate, heavy silicones, algae extract | Moisturisers, SPF, primers | Check ingredients on CosDNA.com |
| Milia | Very heavy occlusive creams, thick overnight masks | Rich eye creams, heavy face masks | Use lighter formulas around eye area |
| Keratosis Pilaris | Physical scrubs, sodium lauryl sulphate, harsh foaming cleansers | Foaming face washes, exfoliating scrubs | Switch to sulphate-free gentle cleanser |
| Textural Dehydration | Alcohol-heavy toners, over-exfoliation, skipping moisturiser | Astringent toners, prescription retinoids (early stages) | Add humectant, seal with occlusive |
why you’re still breaking out with a consistent skincare routine covers exactly how to read labels.
One product audit on CosDNA takes two minutes. Most people find their culprit on the first try.
Frequently Asked Questions
-
How do I know if my bumpy skin is closed comedones or milia?
Closed comedones sit in clusters, are flat or barely raised, and appear in the T-zone. They can sometimes be gently extracted. Milia are perfectly round, hard, pearlescent white, and will not come out with squeezing. They appear most often around the eye area and upper cheeks. If it feels bead-like under your finger and has no head, it’s almost certainly milia.
-
Can dehydrated skin cause bumpy texture?
Yes. When the outer layers of skin lack water, the surface becomes irregular and rough-feeling, even without any clogged pores or structural skin conditions. Dehydration-related texture worsens in cold or dry weather and improves with humidity. Humectants like hyaluronic acid and glycerin paired with an occlusive moisturiser address this directly.
-
What skincare ingredients cause small bumps that aren’t pimples?
Coconut oil and isopropyl myristate commonly cause closed comedones. Heavy occlusive eye creams are a primary trigger for milia. Sodium lauryl sulphate and harsh physical scrubs worsen keratosis pilaris. Alcohol-heavy toners and over-exfoliation can trigger textural dehydration. The ingredient matters as much as the product type.
-
Is keratosis pilaris on the face the same as on the arms?
It’s the same underlying condition (excess keratin blocking hair follicles), but facial skin is thinner and more sensitive than arm skin. The same treatment you’d use on your arms, like a rough body scrub or high-concentration urea cream, can be too harsh for your face. Lactic acid in a gentler concentration is the more appropriate approach for facial KP.
-
How long does it take to see results?
Dehydration-related texture can improve within one to two weeks with the right moisturiser. Closed comedones typically respond to BHA treatment within four to eight weeks. KP is slower. Most people see a noticeable shift after eight to twelve weeks of consistent lactic acid use. Milia that are left alone can resolve within a few weeks to a few months.
-
Can bumpy skin texture appear after starting retinol?
Yes, bumpy texture after starting retinol is completely normal & it’s usually purging. skin purging vs breakout explains exactly how to tell them apart.
-
Should I stop moisturising if I have closed comedones?
No, but change your moisturiser. Skipping moisturiser makes most skin concerns worse over time. The fix is a non-comedogenic formula without pore-clogging ingredients. Check the ingredient list of your current product on CosDNA.com before assuming moisturiser itself is the problem.
-
What causes small white bumps on the face that aren’t acne?
Small, hard, round white bumps that won’t respond to squeezing are almost always milia. Flat white or flesh-coloured bumps in clusters around the T-zone are more likely closed comedones. Rough sandpaper texture across the cheeks points more to keratosis pilaris. Location, texture, size, and whether there’s any kind of opening are the key distinguishing factors.
-
Is rough bumpy skin texture permanent?
Keratosis pilaris is a genetic condition with no permanent cure, but it can be managed effectively with consistent treatment. Milia and closed comedones resolve completely with the right approach. Textural dehydration is fully reversible. For most people, rough bumpy skin texture can be significantly reduced, even if the underlying tendency for KP never fully disappears.
-
When should I see a dermatologist about bumpy skin texture?
See a dermatologist if bumps are painful, cystic, or leaving marks. Also go if you’ve followed the correct treatment for your bump type for 8 to 12 weeks with no change at all. Some conditions need prescription-strength treatment or professional extraction that skincare products alone can’t provide.
The Bottom Line
Rough bumpy skin that isn’t acne is one of the most common and most mishandled skin concerns. The skin texture not pimples conversation needs to start with identification, not with whatever product is on sale this week.Once you know which type you’re dealing with, the right fix becomes clear.
Closed comedones need BHA and a product audit. Milia need patience and professional extraction if they don’t shift on their own. Keratosis pilaris face treatment centres on lactic acid and gentleness over time. And textural dehydration needs water, not more scrubbing.
With consistent treatment and the right ingredients, rough bumpy skin texture genuinely improves. Start with identification. Match the treatment to the type. Give it time.
Related Articles
- Skin purging vs breakout — if you’ve started a new active ingredient and your skin has worsened, this tells you whether it’s a normal adjustment phase or a sign to stop the product
- Why you’re still breaking out with a consistent skincare routine — covers hidden triggers like pore-clogging SPF, dirty pillowcases, and conflicting actives that most guides skip
- Morning skincare vs night skincare — how to layer humectants, occlusives, and actives correctly so they absorb and work properly
- Cleanser causing skin redness— How to know if your cleanser suits your skin & if it irritates then which ingredients to check in it
- Non-Comedogenic Product Might Still Break You Out— A complete guide on non comedogenic & all the myths revolving around it
Sources
- Patient.info—Milia: causes, symptoms, and treatment
- DermNet NZ— Milia: dermatology reference
- DermNet NZ— Comedones and congested pores
- StatPearls / NIH— Keratosis Pilaris: prevalence, diagnosis, and treatment
- American Academy of Dermatology— Keratosis Pilaris: overview and treatment
- PubMed— Salicylic acid: keratolytic mechanism and comedone treatment
- PubMed — Alpha-hydroxy acids and keratin softening in follicular conditions
- AAD— Skin hydration: what dermatologists recommend
- CosDNA— Comedogenicity and irritancy ingredient checker
About the Author
Hi, I’m Sidra.
I’m not a dermatologist or any kind of skincare pro, I’m just someone like you, who got sick of constantly switching up products and never having a clue what was really working. After years of trial and error, I decided to focus on one thing: consistency.
I test routines on myself, I track results in detail, and I write about what realistically shifts and what doesn’t. My aim is to dispel hype and discuss skin-care the way I would with a friend: practical, honest, and backed by patience instead of promises.
Skin type: Normal to dry skin with mild sensitivity
The information in this article is for educational purposes only and does not replace professional dermatological advice. If you have a specific skin condition or concern, please speak with a qualified healthcare provider.